


Mental Health Recommendation & Intervention: Narcissistic Personality Disorder
2 Subjects and their intersectionality of narcissistic co-feeding behavior with mental health and law enforcement engagement.

Synopsis:
NPD stands for Narcissistic Personality Disorder, a mental health condition characterized by a pervasive pattern of grandiosity, a constant need for admiration, and a lack of empathy for others. Individuals with NPD often have an exaggerated sense of their own importance, a preoccupation with fantasies of unlimited success, and a belief in their unique or special status. They may exploit others for personal gain, lack genuine empathy, and have difficulty maintaining healthy relationships. Diagnosis and treatment typically involve mental health professionals.
Clinical Definition:
Narcissistic Personality Disorder (NPD) is a mental health condition characterized by a pervasive pattern of grandiosity, a constant need for admiration, and a lack of empathy. It is part of the Cluster B personality disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). To be diagnosed with NPD, an individual must exhibit a specified number of symptoms, including an exaggerated sense of self-importance, fantasies of unlimited success or power, a belief in their own uniqueness, a preoccupation with fantasies of success, a sense of entitlement, interpersonally exploitative behavior, a lack of empathy, envy of others or a belief that others are envious of them, and arrogant or haughty behaviors and attitudes. The symptoms should be enduring and cause significant distress or impairment in social, occupational, or other important areas of functioning. Diagnosis and treatment are typically carried out by mental health professionals.
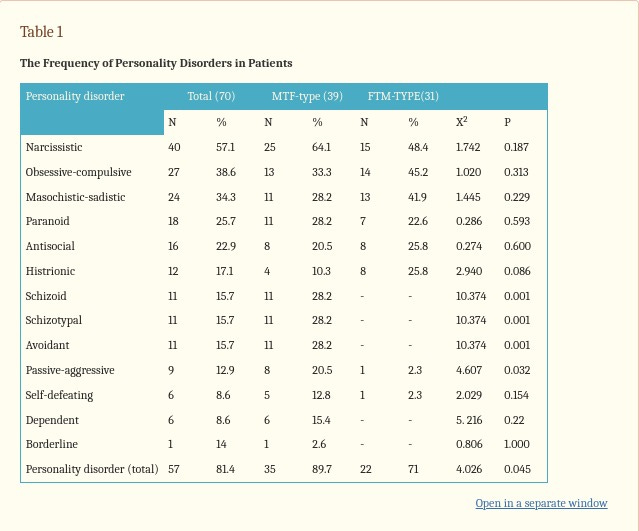
According to Azadeh Mazaheri Meybodi, Ahmad Hajebi, and Atefeh Ghanbari Jolfaei of the Medical Journal of the Islamic Republic of Iran state, “The most frequent personality disorder was narcissistic personality disorder (57.1%) and the least was borderline personality disorder. The average number of diagnoses was 3.00 per patient,” (September 2014). This coincides with much of what is being observable through social media interactions by those who either identify as transgender or those who have a diagnosis of gender dysphoria. However, what is observable on social media does not always translate into every day life outside of that scope. With this in mind, this will be held within the scope of social media and we will be taking a more in-depth look at it.
Subject 1:
Subject 1 is an approximate ##-year old transsexual male-to-female who has recently been discovered to be manipulative, lying, controlling, abandoning a child and sexually assaulting people. The subject displayed grandiose, lack of empathy, manipulative behavior, and need for admiration.
Grandiose – Subject consistently pointed out how a member of the online community dubbed him as the “Pillar of the Community,” and in such manner took this as being a carte blanche to act as the subject pleased.
Lack of Empathy – During a period while a group of individuals were harassing and bullying another group of individuals that the subject was a part of, it was not until much later that the subject later stood up for them after being called out for it, and that it actually made subject perception look unempathetic.
Manipulative Behavior – Subject manipulated women, lesbian women and other transgender individuals into having sex, controlling them, controlling the narrative, deceitfulness, collection of women, exaggerating sexual conquests and a lot more.
Need for Admiration – Subject often took to social media, and even once claiming to have been sexually assaulted. Later found that the sexual assault was a co-opted story from someone else. Then the idea of the “Pillar of the Community” bestowed on him by a known figure to social media made this idea that he was untouchable. Also, and recently, subject claimed to be hospitalized with suicide ideation as a way to garner a sympathetic tone for a recently outing of subjects behavior publicly.
Based on the continued pattern of NPD as a comoribid system of gender dysphoria, it is concluded that subject does have many traits of narcissistic personality disorder and should be in the care of mental health professionals. However, this is not believed to be the case as the subject’s behavior otherwise dictates that this was not what truthfully happened. Knowing suicide protocol, and if they subject had attempted suicide, the idea is to have removed all stressors from subject and placed on a 72-hour psychiatric hold awaiting further evaluation. The subject only stated that they called from a hospital and the only point of contact was a female roommate who could have possibly been manipulated by the subject to comply. This subject also has been known to sexually assault nonreciprocating victims and to have locked others in rooms for as much as 3 days according to inside sources that are unnamed.
Conclusion: This subject is a danger unto them self and to their community.
Subject 2:
Subject 2 is an approximately ##-year old male-to-female who displays a much lower form of NPD, but also enables those who show the normal traits of NPD.
Loyalty Despite Evidence – The invincible Ignorance Fallacy – Denying the evidence that Subject 1 is a sexual predator, has harmed others, denies others claims, and deflective and dismissive.
Avoidance of Accountability – Refuses to accept responsibility, enables Subject 1’s continued behavior, but also not a victim, will not address the issue but rather is dismissive of others claims even with evidence.
Selective Perception – Only sees the good of what Subject 1 has done and refuses to see the negative impacts that Subject 1 has had on the community and the physical and mental health of others affected by their behavior.
Fear of Repercussions – Social media is highly dynamic, and the fear of retribution and repercussions is very high. However, there is no evidence that there are any possibility of repercussions so long as Subject 2 shows their continued support of Subject 1.
There are several issues with Subject 2 if there is a perceived inception to their personal belief system, that the subject lashes out at individuals who do not fit their idealistic views. And to control their perception, a narrative is created in their mind to fit their belief that everyone is lying to them, or in mental health terms, paranoia. The subject then creates this narrative, fills in the gaps in what the believe to maintain control and nothing the subject of their ire may do will deter this newfound belief even when confronted with evidence. This type of person is not dangerous, however this person does need to be in a therapeutic system to maintain a normal sense of mental balance.
Conclusion: Subject 2 should be seen on a regular basis until a possible conclusive termination is determined by both Subject 2 and the mental health professional
Need for Professional Intervention: Both Subject 1 an Subject 2 could benefit from continued professional mental health intervention. Subject 1’s departure from social normalcy and narcissistic behavioral issues should suggest an institutionalized treatment and court mandated probationary period to be determined by the court and mental health professionals. Subject 2 would benefit with regular therapies ongoing with a mental health professional with no other interventions necessary.
Complex Dynamics: Subject 1 and Subject 2 should not be allowed to communicate as each seems to feed off each others dynamics and continued enabling behavioral patterns. Continued contact will only strengthen their bond of co-conspiracy and control of their narrative and narcissism. This connection, when broken, would then allow each to focus on their mental health individual rather than their continued enabling behavior.
Works Cited:
Meybodi, A. M., Hajebi, A., & Jolfaei, A. G. (2014). The frequency of personality disorders in patients with gender identity disorder. Medical journal of the Islamic Republic of Iran, 28, 90.